Understanding ACL Injuries




Author / Lauren Deya
Deya is former professional aerobics and rhythmic gymnast, who works as one of our physical therapists at UP Clinic. With a background in sports – she also played volleyball in University, and now does CrossFit, Boxing and more – she’s seen, and experienced, her fair share of injuries. We spoke to her a few months ago on her personal store [Q&A: Deya (Physical Therapist)], but wanted to learn more about one specific type of injury we see a lot at UP: ACL Injuries.
Read on to learn more about this type of injury and how to manage, and treat it should it happen to you, or someone you know!
Q Deya, you’ve had your own fair share of injuries all over your body – from ankle sprains to your patella, from hip impingement to a tear in your rotator cuff… and more! While we don’t wish pain on anyone, how do you feel your experiences have helped you and your treatment with patients?
With active patients, I understand their willingness to be more fit, or to keep moving. I can help them by showing them how to move well, and not worrying too much about the imagery they see [on an MRI for example], or what you see is negative. I’ve even had surgery on my big toe and so I can relate to that feeling after surgery – feeling helpless.. I know what kind of words to use with my patients to help them continue to build confidence and that they will be okay. For most post-op patients, especially on ligaments, there are still many things you can continue to do after surgery.
That’s ultimately the goal of the surgery right? To restore the function – it’s just doing it in a safe way.

Q So true! Let’s talk about ACL (anterior cruciate ligament) injuries. This is a pretty common, and pretty big, injury right?
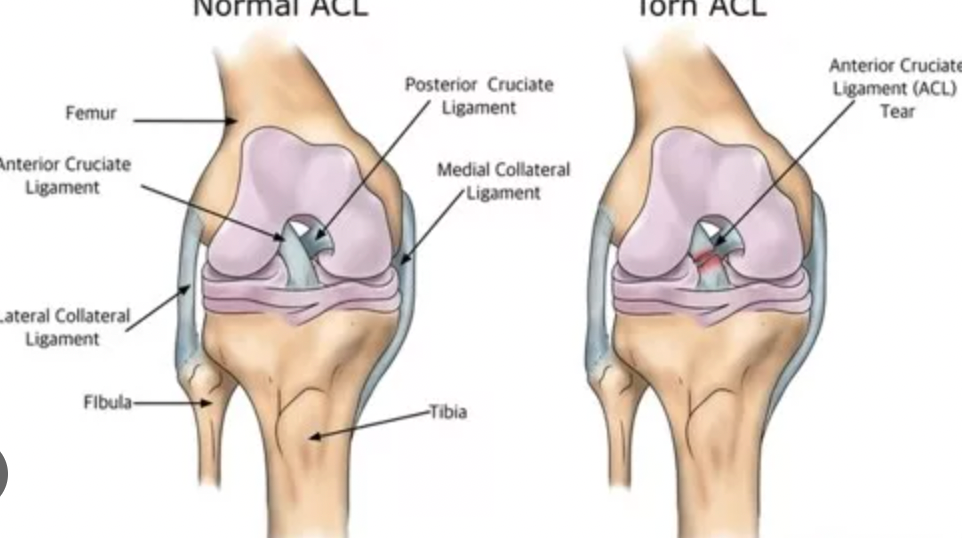
The ACL is a key ligament that helps stabilize the knee joint, connecting the femur to the tibia. When an ACL injury occurs,people may hear a “pop” and then fall down and have difficulty to move (ACL don’t causing much pain but causing the feeling of instability). An ACL injury might not present more than just the feeling of instability. If the injured area is severe and swollen, they need to get checked immediately to make sure the bones are okay.
If they get an MRI report, their doctor needs to determine if they need to do surgery ASAP, or if they can wait, even for a few months. If the doctor says they can wait on the surgery, then it’s important to work with a therapist to do pre-habilitation, which can help them to walk with ma normal gait and perform exercise before the surgery. If they just lie in bed and wait for the surgery, it’s very difficult to get back to the normal gait and function.
I’ve seen all types of patients – some with very low function who don’t want to move, and some who are really ready to get back to action.
People may hear a “pop” and then fall down and have difficulty to move (ACL don’t causing much much but causing the feeling of instability)

Q When you work with a patient who suffers from an ACL injury, what are some of the things you would typically do?
We have a full protocol for the patient. Firstly, we focus on the protocol for them to achieve a particular goal. That said, it really depends on the patient. If they are very active, they might have anxiety about getting back to their sport. If they have no patience with their recovery, we will tell them they are doing great, but also maybe they need to take it slow and steady; not move too fast too soon. If they are less active, and they’re already stiff and stuck in the range of motion, we encourage them actually to move a lot, move better and with better quality. And also explain, why it’s important. We need them practice on their own so they can move back to their regular function. Essentially the protocol is the same for everyone, but the words we use are different.
It’s also important to help motivate the patient during the rehab process. For some patients they might feel helpless. We have to find a way to motivate them to get back to their regular daily life and things they love. We have to help them find goals that they can achieve and encourage them, step-by-step, to move forward.
Q How long does the recovery period typically take?
Our protocol is essentially a guideline on how much they can do. It really depends on how the injury happened and also the patient’s habits. If they have a meniscus replacement with the ACL repairment with meniscus repairment, it can take longer to have a normal gait. If it’s only the ACL the patient should be able to walk normally, post surgery, and after working with us for about six weeks. However, if the patient wants to return to their normal sports, they need to be patient. The ligaments will be very weak within the first three months after the surgery, and it can be very dangerous to do quick lateral movements. It’s possible, but it’s a high injury risk. For safety in sport, it can be about six months, and still doing physical therapy protocol. But just walking normally is a much faster turn around time.

Q Is it also true that there are more ACL injuries in females than in males?
Females are more likely to suffer from ACL injuries because of the way their bones and ligaments are structured. It’s easier for their ligaments to lengthen due to estrogen. Honestly speaking, I don’t know why there’s no protocol specific to females to prevent this injury … probably because most of the studies are based on males in sport. I think it would be incredibly helpful to have a protocol for focusing just on females in sports to prevent injury risk.

Q Is there anything that we can do to prevent the risk of injury?
Move well. The functional movement risk protocol actually describes how best to move. You can have a higher risk doing certain movements, especially if your body is imbalanced. You need to have good muscle strength and coordination, range of motion and balance. Not just practice strength or stretching; not just focus on the movement pattern. You have to have the ability to do it! Your body innately knows how to move but you need to learn how to move efficiently and safely to prevent yourself form injury.
Your body innately knows how to move but you need to learn how to move efficiently and safely to prevent yourself form injury
Q Do you have any examples of patients that you have worked with who have dealt with this injury? And how did you work together?
I’ve been working with a patient who is a student athlete. He had ACL and meniscus replacement surgery 15 months prior, but [the area] is still swollen. So it’s pretty bad. Even since the surgery, he still can’t walk with his normal gait. This was partially because it was during the pandemic so he didn’t get a lot of post-surgery rehabilitation. He still struggles with his range of motion and movement, but he really wants to get back to running, so we’ve tried a lot of things to increase his balance and correct his gait over the last few months.
He used to be a javelin athlete but he can’t do that anymore. So he transitioned to playing cricket. I actually went to his university to see his teammates, how they train and what kind of movements he needs during this game. I tried to learn how to play cricket so I could better help him. (It’s very difficult for me haha). But trying to analyze all the different abilities he needs to complete this type of sport is so important.
He also has a tibial plateau fracture too so there’s a lot of difficulties we’ve had to work through. Even the imagery on the MRI is not super clear because of the metal plate they inserted, which has also made it hard to understand what the deeper reason is behind the swelling. However, with the work we’ve been doing, we‘ve been able to see improvement, especially the gait and range of motion. We found the tibia plateau rotation is what’s prevented him from getting to his normal gate. (When you extend your knee you internally rotate it, when you flex it you externally rotate it a little bit). He cannot do this movement so we are training very, very tiny movements to help him get better.
After working together for a few months, his gait has pretty much returned to normal, which is a huge accomplishment!

Q Wow! The fact that you also went out to his training to learn more about the types of movements he needs to perform also says a lot about your character! You also mentioned another story you wanted to share?
Yes – I have a very young, female patient, who’s very active. She’s an amateur figure skater. She has an ACL and meniscus injury from a long time ago – maybe three years prior. She didn’t do surgery as she didn’t feel it was necessary, but worked with (therapists) Cory and Julie previously before me. With them, she did a lot of exercises to stabilize her knee and hip. It actually worked really well so that she didn’t have to do the surgery until this February, after she then dislocated her patella.
The interesting part is the surgeon decided not to do anything for her ligament. He just fixed the meniscus. Because she is a very active young lady, and is very flexible. Her range of motion after the surgery is pretty good. Eight weeks after her surgery she can already do a normal gait, and she’s been able to travel and can really control her body. I’m still not clear as to why the surgeon didn’t touch her ACL and help her stabilize the knee, and only focus on the meniscus, but she is still doing really well. Possibly because of all the work she has put into her recovery!

Q What great success stories! Do you have any advice for someone who experiences trauma in the knee and is unsure if surgery is necessary?
I have seen some patients who just want to do a non-surgical ACL rehab. All surgeons will tell them they need to do a surgery. I would encourage this type of patient to try rehabilitation first to see if the knee pain really comes from an ACL injury or it’s more like patella syndrome or something else. Some people are just born with looser ACLs, some are born with tighter ones… if you haven’t noticed your ACL was injured before, and you have knee pain, but it’s not from a serious trauma or accident, you should really check with the physiotherapist first to see if surgery is necessary, or if we can do something to help you without going through surgery.
I have one patient who was told to lie in bed for four weeks, and after that her knee became swollen and she had muscle atrophy. She couldn’t even walk properly and all the surgeons advised her to do the surgery. She came to me and I checked and yes, it was a little loose, but when we checked the other leg it was very similar so it’s hard to say if that’s just how she was born or if it was a small injury to the ACL, but just not that serious. After working together she’s doing great now.
I think it’s really important to encourage patients to do whatever they want after rehabilitation. A lot of my patients I have, the surgeon will tell them they cannot continue their sports. It gives patients anxiety or makes them worried about their life; they get a fear of movement. These types of words makes them feel even more disabled. We need to be very careful with our wording, because these types of words can enhance their suffering. As long as they have the right ways of exercising and the right way to follow a rehabilitation process, the patient should be able to do whatever they want. That’s why we are here.

本篇文章来源于微信公众号: 上海优复门诊部